

")
Stroke
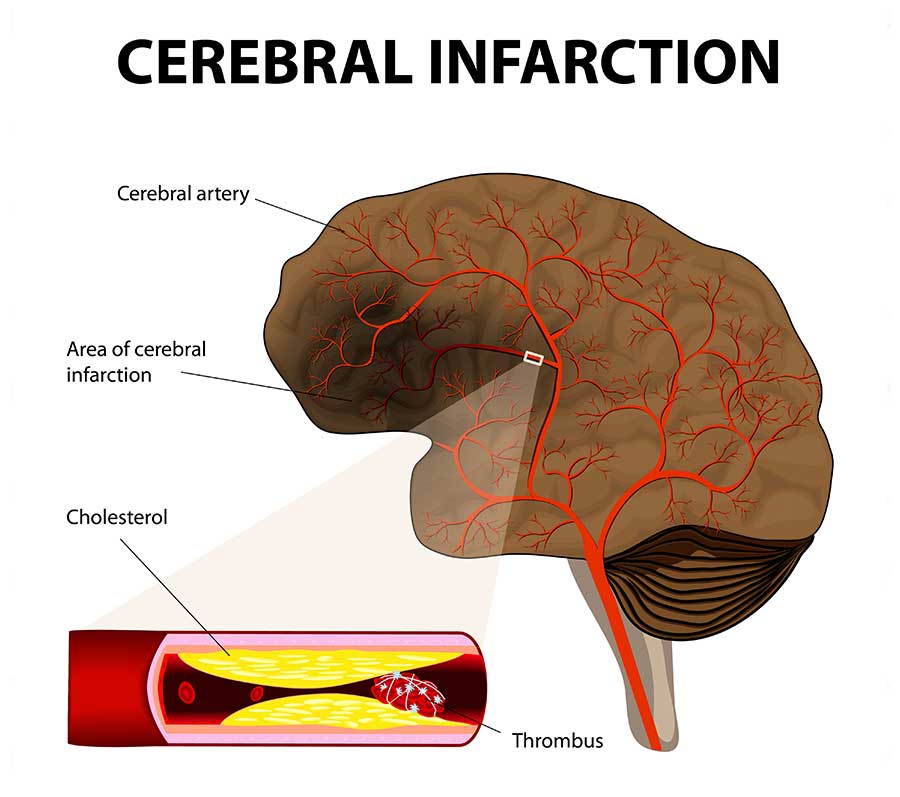 The faster an acute stroke is treated, the less permanent is the damage. That's where the maxim "Time is Brain" comes from. The brain tissue, which no longer receives sufficient oxygen due to a vascular occlusion, should be resupplied with blood by thrombolysis or thrombectomy before it dies.
The faster an acute stroke is treated, the less permanent is the damage. That's where the maxim "Time is Brain" comes from. The brain tissue, which no longer receives sufficient oxygen due to a vascular occlusion, should be resupplied with blood by thrombolysis or thrombectomy before it dies.
As signs of a stroke, several symptoms can occur suddenly, and, depending on the severity, also simultaneously:
- numbness in the face, an arm, leg or an entire side of the body,
- confusion, speech or word finding, writing or comprehension disorder,
- swallowing disorders (dysphagia),
- painless visual disorder in one or both eyes, one-sided pupil dilation, visual field failure, double vision,
- vertigo, gait disturbance, balance or coordination disorder (ataxia),
- lack of perception of part of the environment or of one's own body,
- disturbed consciousness (somnolence, coma), orientation disorders,
- severe headache, nausea and vomiting,
- may indicate a cerebral hemorrhage.
An acute stroke is an emergency case and must be immediately treated in the hospital (s. below in-hospital acute treatment). After a stroke, further neurological care is usually necessary, for example, for pharmacological therapy, for palsies, or for epileptic seizures.
Transient ischemic attacks (TIA) are short blood supply disorders that result in temporary neurological deficits. As they are harbingers of stroke, further examinations must be carried out in order to minimize the risk of a subsequent stroke. In the case of narrowed brain-supplying arteries (e.g. carotid stenosis), regular checks by means of state-of-the-art ultrasound procedures are carried out in our practice in order to prevent a stroke, but also to prevent unnecessary procedures on the blood vessels (s. below color-coded Doppler and duplex sonography of the neck vessels and brain arteries).
